Millions of people experience a life-threatening bleed each year due to an accident or injury, chronic disease, or as an uncommon but significant complication of medicines such as blood thinners.1-3 Management of these bleeds often requires a range of specialists including emergency care clinicians, haematologists, cardiologists, internists, surgeons and pharmacists to coordinate potentially lifesaving treatment in the emergency care setting.4
What is uncontrolled bleeding?
If not effectively managed in the emergency setting, major bleeds can cause serious complications and become life threatening.5 These types of uncontrolled bleeds have led to more than 450,000 deaths globally each year, making it a priority condition to quickly and efficiently manage.6
Uncontrolled bleeding has several underlying causes
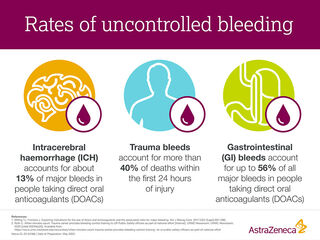
There are many reasons someone may experience a life-threatening bleed, ranging from chronic risk factors or a one-time accident or surgery. 5,7 This type of bleeding can happen externally due to lacerations, cuts or punctures, or internally within the body such as inside the brain tissue (intracerebral), skull (intracranial) or gastrointestinal (GI) system.5,7
Physical trauma, such as a car accident, can cause bleeding at critical sites either internally and/or externally.2 People with a potentially higher risk for a bleed include those with chronic conditions.8-12 Certain diseases such as cardiovascular disease, hypertension, Crohn’s disease and irritable bowel syndrome can increase someone’s risk of experiencing bleeding.8-12 Genetic disorders such as haemophilia can also result in uncontrolled bleeding.13
While caring for patients with other cardiovascular conditions and risk factors, clinicians often prescribe blood thinners.14 People with deep vein thrombosis, pulmonary embolism and atrial fibrillation may take these medicines to keep their blood from coagulating and forming clots, which can obstruct blood flow and potentially harm different organs in the body such as the brain, lungs, and heart.14,15
Clinicians prescribe a variety of blood thinners including warfarin and direct oral anticoagulants (DOACs).16 While DOACs are effective and convenient medications and although their benefits outweigh the risks, they carry a small but significant risk of a major bleed developing such as an intracerebral haemorrhage (ICH), GI or non-ICH trauma bleed since the blood is less able to clot.16-18 It is vital medics can coordinate potentially lifesaving care in the emergency setting for these patients.
Emergency clinicians face many challenges while managing uncontrolled bleeds
After a patient arrives at the hospital with a major bleed, emergency medicine clinicians (EMCs) must evaluate whether the patient meets the criteria for a certain care management option.5 Time is of the essence and EMCs must triage and work quickly to implement a strategy.5
Several medical associations including the American College of Cardiology, European Society for Emergency Medicine and American College of Emergency Physicians have established guidelines to help EMCs and hospitals create a management strategy.4,19-20
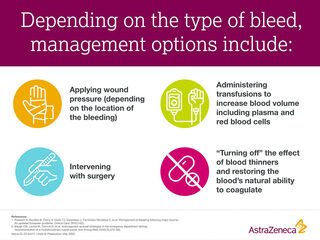
While all patients experiencing a major bleed require quick attention, it’s vital to specifically identify the patients on anticoagulants.4 These medicines inhibit the body’s natural clotting ability, making it more difficult to manage uncontrolled bleeding.14
To help estimate the risk of major bleeding for patients on blood thinners, a patient’s medical history is reviewed to identify hypertension, abnormal liver or renal function, previous strokes, bleeding history or predisposition, labile INR, age (determine if they’re over the age of 65) and drug or alcohol usage.21 This method is a tool called HAS-BLED and can predict the risk of major bleeding for patients on blood thinners.21 In urgent settings, friends and family members can also provide medical information and help identify those on blood thinners.
Transforming the management of uncontrolled bleeding
Managing uncontrolled bleeding is complex and requires the coordination of care across multiple specialties including emergency medicine clinicians, haematologists, cardiologists, neurologists, surgeons and more.4
The care provided in the emergency setting can be complex, involving rapid decision-making and careful coordination. Guideline-based hospital protocols are vital tools to help cross-disciplinary teams deliver care that could ultimately save a life.
To help all these groups work together, it’s important to establish clear hospital protocols based on pre-existing guidelines that can help clinicians deliver lifesaving care to patients suffering from uncontrolled bleeds. These clinical tools can facilitate information sharing across multidisciplinary teams and help practitioners deliver safer, more effective care. It is also important to establish, whenever possible, dedicated stewardship programs that drive the development, implementation, consistent application, evaluation of care and education of these protocols and guidelines.
At AstraZeneca, we’re committed to transforming care for patients living with cardiovascular, renal and metabolic diseases and highlighting their undertreated and interconnected events such as uncontrolled bleeds. Early detection and care are critical to improving patient outcomes and reducing the burden of cardiovascular, renal and metabolic (CVRM) diseases and their related risks and complications for patients, societies and our planet.
You may also like



References
1. American Heart Association [Internet]. 2021 Heart Disease & Stroke Statistical Update Fact Sheet Global Burden of Disease. 2021; [cited 2023 Apr 28]. Available from: https://professional.heart.org/-/media/PHD-Files-2/Science-News/2/2021-Heart-and-Stroke-Stat-Update/2021_Stat_Update_factsheet_Global_Burden_of_Disease.pdf.
2. Cleveland Clinic [Internet]. What are the most common causes of hemorrhage? 2023; [cited 2023 Apr 28]. Available from: https://my.clevelandclinic.org/health/symptoms/21654-hemorrhage#possible-causes.
3. Dhakal P, et al. Reversal of anticoagulation and management of bleeding in patients on anticoagulants. Clin Appl Thromb Hemost. 2017;23:410-415.
4. Baugh CW, Levine M, Cornutt D, et al. Anticoagulant reversal strategies in the emergency department setting: recommendation of a multidisciplinary expert panel. Ann Emerg Med. 2020;76:470-485.
5. Donley ER, et al. [Internet]. Hemorrhage control; [cited 2023 Apr 28]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535393/. February 12, 2023.
6. World Health Organization [Internet]. Uncontrolled Bleeds. 2020; [cited 2023 Apr 28]. Available from: https://www.who.int/home/search?indexCatalogue=genericsearchindex1&searchQuery=uncontrolled%20bleeding&wordsMode=AnyWord.
7. Johnson AB and Burns B [Internet]. Hemorrhage; [cited 2023 Apr 28]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542273/. February 15, 2023.
8. Kaikita K, et al; on behalf of the AFIRE Investigators. Bleeding and subsequent cardiovascular events and death in atrial fibrillation with stable coronary artery disease. Circ Cardiovasc Interv. 2021;14:e010476.
9. Hasegawa S, et al. Association between diabetes and major bleeding complications of renal biopsy. Kidney Int Rep. 2022;7:232-240.
10. Mayo Clinic [Internet]. High blood pressure dangers: hypertension’s effects on your body. 2022; [cited 2023 Apr 28]. Available from: https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/in-depth/high-blood-pressure/art-20045868.
11. Kim E, et al. Life-threatening lower gastrointestinal hemorrhage in pediatric Crohn’s disease. Pediatr Gastroenterol Hepatol Nutr. 2013;16:53-60.
12. Fashner J and Gitu AC. Common gastrointestinal symptoms: irritable bowel syndrome. FP Essent. 2013;413:16-23.
13. National Institutes of Health [Internet]. Bleeding disorders: causes and risk factors; [cited 2023 Apr 28]. Available from: https://www.nhlbi.nih.gov/health/bleeding-disorders/causes.
14. Compton K [Internet]. Blood thinners. 2022; [cited 2023 Apr 28]. Available from: https://www.drugwatch.com/health/cardiovascular-health/blood-thinners/.
15. Cleveland Clinic [Internet]. Blood clots; [cited 2023 Apr 28]. Available from: https://my.clevelandclinic.org/health/diseases/17675-blood-clots.
16. Chen A, et al. Direct oral anticoagulant use: a practical guide to common clinical challenges. J Am Heart Assoc. 2020;9:e017559.
17. Milling TJ, Frontera J. Exploring indications for the use of direct oral anticoagulants and the associated risks of major bleeding [Internet]. The American journal of managed care. U.S. National Library of Medicine; 2017 [cited 2023Mar16]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5568002/
18. Kauvar DS, Wade CE. The epidemiology and modern management of traumatic hemorrhage: US and International Perspectives [Internet]. Critical Care . BioMed Central; 2005 [cited 2023Mar24]. Available from: https://ccforum.biomedcentral.com/articles/10.1186/cc3779
19. Tomaselli GF, et al. 2020 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76:594-622.
20. Spahn DR, Bouillon B, Cerny V, Duranteau J, Filipescu D, Hunt BJ, et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition - critical care [Internet]. BioMed Central; 2019 [cited 2023 May 15]. Available from: https://ccforum.biomedcentral.com/articles/10.1186/s13054-019-2347-3
21. Zhu W, He W, Guo L, et al. The HAS‐BLED score for predicting major bleeding risk in anticoagulated patients with atrial fibrillation: a systematic review and meta‐analysis. Clin Cardiol. 2015;38:555-561
Veeva ID: Z4-49282
Date of preparation: May 2023