Subgroup analysis from the Phase III THALES trial showed treatment effect in easy-to-identify patient population
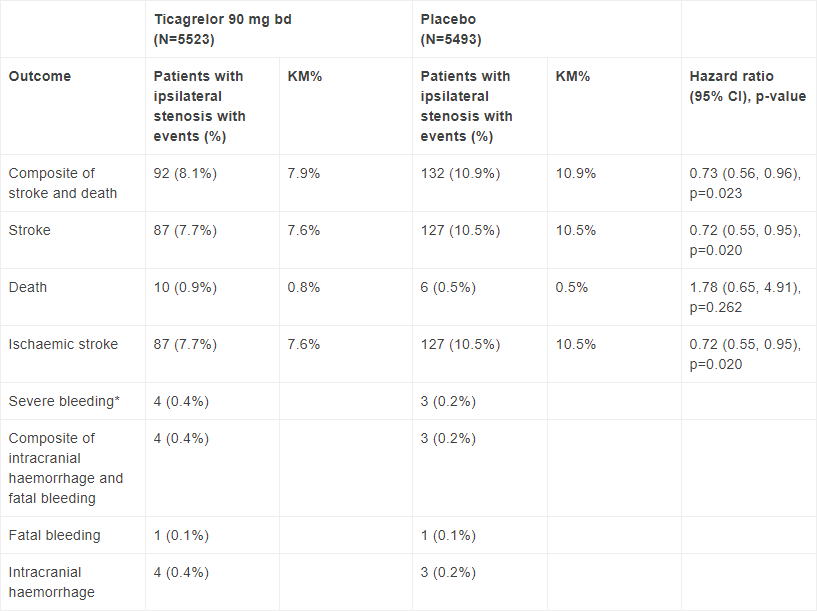
Detailed results from a prespecified subgroup (n=2,351) analysis of the positive THALES Phase III trial showed AstraZeneca’s Brilinta (ticagrelor) 90mg used twice daily and taken with daily aspirin for 30 days reduced the rate of the composite of stroke and death by 27% (absolute risk reduction 3%, HR 0.73 [95% CI 0.56, 0.96], nominal p=0.023) compared to aspirin alone in patients who had an acute ischaemic stroke or a transient ischaemic attack (TIA) and had ipsilateral atherosclerotic stenosis in the head and neck (cervicocranial) arteries.1 This means that the number needed to treat (NNT) was 34 in this sub-group of patients compared to a NNT of 92 in the overall THALES population.1,2 This represents a consistent reduction in an easily identifiable patient population.
In the subgroup of patients without ipsilateral stenosis at baseline, the rate of the primary composite endpoint of stroke or death was 4.8% for the aspirin and ticagrelor group versus 5.3% for the aspirin alone group (HR 0.89 [95% CI 0.74, 1.08]).1 Furthermore, aspirin plus ticagrelor also reduced the rate of the first secondary endpoint of ischaemic stroke by 28% (absolute risk reduction 2.9%, HR 0.72 [95 % CI 0.55, 0.95], nominal p=0.02) compared to aspirin alone up to day 30 in this sub-group.1
Atherosclerotic stroke or TIA can occur when a lipid-rich plaque ruptures in head and neck arteries leading to the formation of blood clots that may obstruct the blood flow to the brain. About 40 per cent of patients with ischaemic stroke have an ipsilateral (on the same side as the symptomatic cerebral ischaemia) atherosclerotic stenosis (narrowing of the arteries due to plaque formation), which may cause a stroke.1
Dr Pierre Amarenco, International Coordinating Investigator and Vice-Chair of the THALES Executive Committee and Professor of Neurology at Paris University, said: “A body of scientific evidence, including our own analysis, shows that patients with ipsilateral atherosclerotic disease experience a much higher risk of ischaemic stroke than patients with other subtypes.1 This new data from the THALES trial indicates that ticagrelor offers protection in this patient population, which is easily identified in clinical practice.”
Mene Pangalos, Executive Vice President, BioPharmaceuticals R&D, said: “Patients who had an acute ischaemic stroke or a transient ischaemic attack are at high risk for recurrent, potentially disabling or fatal events.3 Given this and the established heritage of ticagrelor in the prevention of atherothrombotic events, we are pleased to see that aspirin plus ticagrelor has the potential to be an effective preventive treatment for subsequent stroke in patients with cervicocranial atherosclerosis.”
Key efficacy and safety data from the subgroup analysis of the THALES trial
i. Amarenco P et al. Ticagrelor added to aspirin in acute non-severe ischemic stroke or TIA of atherosclerotic origin. Stroke; doi: 10.1161/STROKEAHA.120.032239.
* By GUSTO (Global Utilization of Streptokinase and Tissue-type plasminogen activator for Occluded coronary arteries trial) definition; CI=confidence interval; KM=Kaplan-Meier
The risk of severe bleeding events in the atherosclerotic subgroup was 0.4% in the aspirin plus ticagrelor arm and 0.2% in the placebo arm.1 The results were in line with the known safety profile of ticagrelor.
Results from the subgroup analysis of the THALES trial were presented on 16 November at the American Heart Association Scientific Sessions 2020 and simultaneously published in Stroke.
Earlier this month, AstraZeneca announced that the US Food and Drug Administration (FDA) approved ticagrelor to reduce the risk of stroke in patients with an acute ischaemic stroke (National Institutes of Health Stroke Scale score ≤5) or high-risk TIA.
Stroke
An ischaemic stroke is caused by a blockage cutting off the blood supply to a region of the brain. A transient ischaemic attack, is a temporary blockage of the blood supply to a region of the brain, resulting in symptoms only lasting for a short amount of time. Stroke is a leading cause of disability and death worldwide.4 In the US, someone has a stroke every 40 seconds, and every four minutes, someone dies of stroke.5 About one in four strokes are recurrent, with the risk particularly high within 30 days after the initial event and even higher when looking at time periods closer to the initial event.6,7
THALES
THALES is an AstraZeneca-sponsored, randomised, placebo-controlled, double-blinded, international, multicentre, event-driven trial involving more than 11,000 patients from 28 countries. It tested the hypothesis whether aspirin plus ticagrelor is superior to aspirin alone in preventing the composite of stroke and death in patients with non-cardioembolic acute ischaemic stroke or high-risk TIA. Patients were randomised within 24 hours of onset of acute ischaemic stroke or high-risk TIA symptoms and treated for 30 days. Study treatments were ticagrelor 180mg loading dose on day 1, followed by 90mg twice daily on days 2–30, or matching placebo. All patients received open-label aspirin 300–325mg on day 1, followed by 75–100mg once daily on days 2–30. The primary efficacy outcome was the time to the composite endpoint of stroke and death at 30 days. The primary safety outcome is time to first severe bleeding event according to the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO) definition, which includes fatal bleedings, intracranial haemorrhage; and bleeding causing hemodynamic compromise requiring intervention. In the overall population ticagrelor taken with daily aspirin for 30 days, reduced the rate of the primary composite endpoint of stroke and death by 17% (absolute risk reduction 1.1%; HR 0.83 [95% CI 0.71, 0.96], p=0.02), compared to aspirin alone.
Brilinta
Brilinta (ticagrelor) is an oral, reversible, direct-acting P2Y12 receptor antagonist that works by inhibiting platelet activation. Ticagrelor together with aspirin, has been shown to significantly reduce the risk of major adverse cardiovascular (CV) events (heart attack, stroke or CV death), in patients with acute coronary syndromes (ACS) or a history of heart attack. In the US, ticagrelor is also indicated for the reduction of the risk of a first heart attack or stroke in high-risk patients with coronary artery disease.
In the EU ticagrelor, co-administered with aspirin, is indicated for the prevention of atherothrombotic events in adult patients with ACS, or for patients with a history of heart attack and a high risk of developing an atherothrombotic event.
AstraZeneca in CVRM
Cardiovascular, Renal and Metabolism (CVRM) together forms one of AstraZeneca’s three therapy areas and is a key growth driver for the Company. By following the science to understand more clearly the underlying links between the heart, kidneys and pancreas, AstraZeneca is investing in a portfolio of medicines to protect organs and improve outcomes by slowing disease progression, reducing risks and tackling co-morbidities. The Company’s ambition is to modify or halt the natural course of CVRM diseases and potentially regenerate organs and restore function, by continuing to deliver transformative science that improves treatment practices and cardiovascular health for millions of patients worldwide.
AstraZeneca
AstraZeneca (LSE/STO/Nasdaq: AZN) is a global, science-led biopharmaceutical company that focuses on the discovery, development and commercialisation of prescription medicines, primarily for the treatment of diseases in three therapy areas - Oncology, Cardiovascular, Renal & Metabolism, and Respiratory & Immunology. Based in Cambridge, UK, AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. Please visit astrazeneca.com and follow the Company on Twitter @AstraZeneca.
Contacts
For details on how to contact the Investor Relations Team, please click here. For Media contacts, click here.
References
1. Amarenco P et al. Ticagrelor added to aspirin in acute non-severe ischemic stroke or TIA of atherosclerotic origin. Stroke. Published online November 16 2020; doi: 10.1161/STROKEAHA.120.032239.
2. Johnston SC, Amarenco P, Denison H, et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. N Engl J Med 2020; 383:207-217.
3. Amarenco P et al. One-Year Risk of Stroke after Transient Ischemic Attack or Minor Stroke. N Engl J Med 2016; 374(16):1533–42.
4. Roth GA et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet 2018; 392(10159):1736–88
5. Virani SS, Alonso A, Benjamin EJ et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation 2020;141(9):e139–e596.
6. Hankey GJ. Secondary stroke prevention. Lancet Neurol 2014; 13(2):178–94.
7. Coull AJ et al. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: Implications for public education and organisation of services. BMJ 2004; 328(7435):326