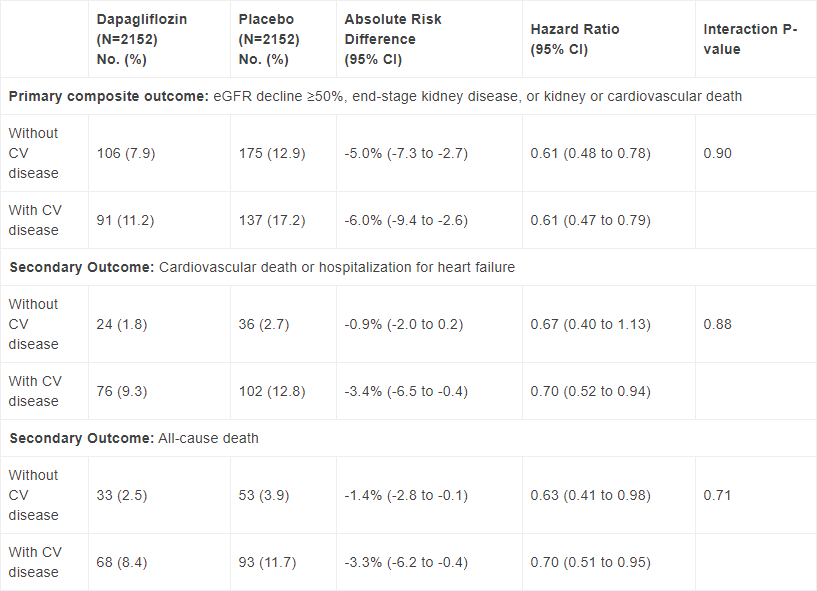
New subgroup analysis data from the DAPA-CKD Phase III trial showed that Farxiga (dapagliflozin) reduced the risk of the primary composite of worsening of renal function or risk of cardiovascular (CV) or renal death by 39% versus placebo in patients with chronic kidney disease (CKD) with and without type-2 diabetes (T2D), irrespective of their CV disease history status. The absolute risk reductions were 5% and 6% respectively, for patients without CV disease at baseline and patients with CV disease at baseline; p-value for interaction = 0.90. 1
The subgroup analysis evaluated the trial’s primary endpoint of worsening of renal function or risk of CV or renal death as well as secondary endpoints in subgroups of patients at baseline without a history of CV disease (“primary prevention” patients, 37.4% of trial participants) and in patients with CV disease (“secondary prevention” patients, 62.4% of trial participants). Compared to the primary prevention patients at baseline, the secondary prevention patients were older, more often male, and smokers, had a higher mean systolic blood pressure, and higher body mass index. Additionally, patients with CV disease were more likely to have T2D than those without CV disease.1
John McMurray, MD, Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, University of Glasgow, UK, and member of the DAPA-CKD Executive Committee said: “These data show that even the most at-risk patients experienced consistent benefit from dapagliflozin, with a reduction of risk for kidney failure, death from cardiovascular causes or hospitalization for heart failure, as well as prolonged survival.”
Mene Pangalos, Executive Vice President, BioPharmaceuticals R&D, said: “This study further emphasises that patients with chronic kidney disease are at a heightened risk of adverse cardiovascular and renal outcomes, including death from any cause. We are excited to see dapagliflozin show consistent benefit in these patients, irrespective of their cardiovascular disease status, and are committed to potentially helping them live longer, healthier lives.”
Primary and secondary endpoints according to baseline cardiovascular disease status.
The safety and tolerability of dapagliflozin were consistent with the well-established safety profile of the medicine.
The data were presented at the American Heart Association 2020 Scientific Sessions and were published in Circulation. Detailed results from the trial were shared earlier this year and published in The New England Journal of Medicine.
Last month, dapagliflozin was granted Breakthrough Therapy Designation in the US for patients with CKD, with and without T2D.
Chronic kidney disease
CKD is a serious, progressive condition defined by decreased kidney function (shown by reduced estimated glomerular filtration rate [eGFR] or markers of kidney damage, or both, for at least three months) affecting nearly 700 million people worldwide, many of them still undiagnosed.2–5 The most common causes of CKD are diabetes, hypertension and glomerulonephritis.6 CKD is associated with significant patient morbidity and an increased risk of CV events,3 such as heart failure (HF) and premature death.7 In its most severe form, known as end-stage kidney disease (ESKD), kidney damage and deterioration of kidney function have progressed to the stage where dialysis or kidney transplantation are required.8 The majority of patients with CKD will die from CV causes before reaching ESKD.9
DAPA-CKD
DAPA-CKD is an international, multi-centre, randomised, double-blinded trial in 4,304 patients designed to evaluate the efficacy of dapagliflozin 10mg, compared with placebo, in patients with CKD Stages 2-4 and elevated urinary albumin excretion, with and without T2D. Dapagliflozin was given once daily in addition to standard of care. Detailed results showed that dapagliflozin reduced the risk of the composite measure of worsening of renal function or CV or renal death (defined as ≥50% sustained decline in estimated glomerular filtration rate (eGFR), onset of end-stage kidney disease (ESKD) or CV or renal death) by 39% compared to placebo (absolute risk reduction [ARR] = 5.3% over the median time in study of 2.4 years; p <0.0001]). The results were consistent in patients both with and without T2D. Dapagliflozin also met all secondary endpoints (renal composite of ≥50% sustained decline in eGFR, ESKD or renal death; composite of CV death and hHF) including significantly reducing the risk of death from any cause by 31% (ARR = 2.1%; p =0.0035) compared to placebo.10
Farxiga
Farxiga (dapagliflozin) is a first-in-class, oral, once-daily sodium-glucose co-transporter-2 inhibitor indicated in adults for the treatment of insufficiently controlled T2D as both monotherapy and as part of combination therapy as an adjunct to diet and exercise to improve glycaemic control, with the additional benefits of weight loss and blood-pressure reduction. In the DECLARE-TIMI 58 CV outcomes trial in adults with T2D, dapagliflozin reduced the risk of the composite endpoint of hHF or CV death versus placebo, when added to standard of care.
In May 2020, dapagliflozin was approved in the US to reduce the risk of CV death and hHF in adults with HF (NYHA class II-IV) with reduced ejection fraction (HFrEF) with and without T2D. Dapagliflozin is currently being tested for patients with HF in the DELIVER (HF with preserved ejection fraction, HFpEF) and DETERMINE (HFrEF and HFpEF) Phase III trials. Dapagliflozin will also be tested in patients without T2D following an acute myocardial infarction (MI) or heartattack in the DAPA-MI trial - a first of its kind, indication-seeking registry-based randomised controlled trial. Dapagliflozin has a robust programme of clinical trials that includes more than 35 completed and ongoing Phase IIb/III trials in more than 35,000 patients, as well as more than 2.5 million patient-years’ experience.
AstraZeneca in CVRM
Cardiovascular, Renal and Metabolism (CVRM) together forms one of AstraZeneca’s three therapy areas and is a key growth driver for the Company. By following the science to understand more clearly the underlying links between the heart, kidneys and pancreas, AstraZeneca is investing in a portfolio of medicines to protect organs and improve outcomes by slowing disease progression, reducing risks and tackling co-morbidities. The Company’s ambition is to modify or halt the natural course of CVRM diseases and potentially regenerate organs and restore function, by continuing to deliver transformative science that improves treatment practices and cardiovascular health for millions of patients worldwide.
AstraZeneca
AstraZeneca (LSE/STO/Nasdaq: AZN) is a global, science-led biopharmaceutical company that focuses on the discovery, development and commercialisation of prescription medicines, primarily for the treatment of diseases in three therapy areas - Oncology, Cardiovascular, Renal & Metabolism, and Respiratory & Immunology. Based in Cambridge, UK, AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. Please visit astrazeneca.com and follow the Company on Twitter @AstraZeneca.
Contacts
For details on how to contact the Investor Relations Team, please click here. For Media contacts, click here.
References
1. McMurray J. Effect of dapagliflozin on clinical outcomes in patients with chronic kidney disease, with and without cardiovascular disease. presented at: AHA Scientific Sessions 2020, November 13–17, 2020.
2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International Supplement 2013; (3):1–150.
3. Bikbov B et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet 2020; 395(10225):709–33.
4. Hirst JA et al. Prevalence of chronic kidney disease in the community using data from OxRen: A UK population-based cohort study. Br J Gen Pract 2020; 70(693):e285-e293.
5. National Kidney Foundation. Kidney Disease: The Basics; 2020 [cited 2020 Sep 23]. Available from: URL: https://www.kidney.org/news/newsroom/factsheets/KidneyDiseaseBasics.
6. National Kidney Foundation. Kidney Disease: Causes; 2015 [cited 23 September 2020]. Available from: URL: https://www.kidney.org/atoz/content/kidneydiscauses
7. Segall L et al. Heart failure in patients with chronic kidney disease: A systematic integrative review. Biomed Res Int 2014; 2014:937398.
8. Centers for Disease Control and Prevention (CDC). Chronic Kidney Disease in the United States, 2019; 2019 [cited 2020 Oct 1]. Available from: URL: https://www.cdc.gov/kidneydisease/publications-resources/2019-national-facts.html.
9. Briasoulis A, Bakris GL. Chronic Kidney Disease as a Coronary Artery Disease Risk Equivalent. Current Cardiology Reports 2013; 15(3):340.
10. McMurray JJV et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019; 381(21):1995–2008.