06 December 2016
First randomised Phase III trial (AURA3) of Tagrisso against chemotherapy
Tagrisso reduced risk of disease progression by 70% and improved progression-free survival (PFS) by almost six months
Patients with central nervous system metastases achieved similar benefit as the overall patient population in pre-specified exploratory subgroup analysis
AstraZeneca today presented data from the AURA3 trial that data is supportive of Tagrisso (osimertinib) potentially becoming the new standard of care for 2nd-line treatment of patients with epidermal growth factor receptor (EGFR) T790M mutation-positive locally-advanced or metastatic non-small cell lung cancer (NSCLC). The first randomised Phase III data showed that Tagrisso 2nd-line therapy improved progression-free survival (PFS) by 5.7 months compared with standard platinum-based doublet chemotherapy (Hazard Ratio [HR]=0.3). The results were presented at the 17th World Conference on Lung Cancer (WCLC) in Vienna, Austria, hosted by the International Association for the Study of Lung Cancer, and published simultaneously online in The New England Journal of Medicine.
Sean Bohen, Executive Vice President, Global Medicines Development and Chief Medical Officer at AstraZeneca, said: “The confirmatory Phase III data suggest the potential for Tagrisso to replace chemotherapy as the standard of care for patients who have progressed following EGFR tyrosine kinase inhibitor treatment. As lung cancer is the most common type of cancer to spread to the brain, it is also encouraging to see the activity of Tagrisso in patients with central nervous system metastases whose prognosis is often particularly poor.”
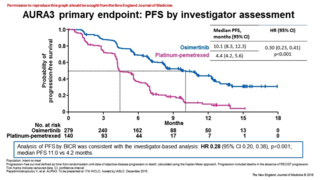
AURA3 data showed Tagrisso offered a statistically-significant improvement in PFS versus standard platinum-based doublet chemotherapy (10.1 months vs 4.4 months, hazard ratio [HR] 0.30; 95% confidence interval (CI):0.23, 0.41; p<0.001). In the 34% of patients with central nervous system (CNS) metastases at baseline, PFS was also significantly greater with Tagrisso than with platinum-based doublet chemotherapy (8.5 months vs 4.2 months, HR 0.32; 95% CI: 0.21, 0.49).
Dr. Vassiliki A Papadimitrakopoulou, from the University of Texas MD Anderson Cancer Center, Houston, Texas, USA, said: “The results of AURA3 are not only statistically significant, but clinically meaningful because it is the first time a targeted medicine like Tagrisso has shown improvement in progression-free survival over standard platinum-pemetrexed chemotherapy. It’s very rewarding to be able to give this type of news to patients, as it highlights the major advances we are making in targeted lung cancer treatments.”
Professor Tony Mok, from the Chinese University of Hong Kong, Hong Kong said: “The superiority of Tagrisso in progression free survival and response rate over platinum-pemetrexed chemotherapy suggests we may be moving towards a new standard of care for patients with resistance to EGFR TKI. With the publication of the AURA3 data, clinicians should perform T790M mutation testing to ensure Tagrisso be given to patients who are most likely to benefit.”
The AURA3 safety data for Tagrisso were in line with previous experience. Grade ≥3 drug-related adverse events (AEs) were reported in 6% of patients (n=16) treated with Tagrisso and 34% (n=46) treated with platinum-based doublet chemotherapy. The most common drug-related AEs in the Tagrisso group, were diarrhoea (29% overall; 1% Grade ≥3) and rash (28% overall; <1% Grade ≥3) and, in the chemotherapy group, they were nausea (47% overall; 3% Grade ≥3) and decreased appetite (32% overall; 3% Grade ≥3).
The data for AURA3 are consistent with those previously presented in the Phase II trials, AURA2 and AURA extension. This consistency extends to testing of tissue and plasma samples for the detection of the EGFR T790M resistance mutation. In AURA3, approximately half of patients with T790M in tumour tissue also had the T790M mutation detected in plasma. Clinical benefits were reported with Tagrisso compared to platinum-based doublet chemotherapy, irrespective of whether the T790M mutation was identified by plasma ctDNA or tissue testing. When feasible, tissue testing is recommended for patients with a negative plasma T790M test.
Tagrisso was granted accelerated approval by the US Food and Drug Administration (FDA) in November 2015 for the treatment of patients with metastatic EGFR T790M mutation-positive NSCLC, as detected by an FDA-approved test, who have progressed on or after EGFR TKI therapy. In the EU, Tagrisso was granted conditional marketing authorisation for adult patients with locally advanced or metastatic EGFR T790M NSCLC, irrespective of previous EGFR-TKI treatment by the European Medicines Agency (EMA) in February 2016.
In addition, Tagrisso received approval in Japan in March 2016 for the treatment of patients with EGFR T790M mutation-positive inoperable or recurrent NSCLC that is resistant to EGFR TKI therapy, and it is currently under fast track review in China, where nearly half of lung cancer patients are thought to have the EGFR mutation.
NOTES TO EDITORS
To view and download additional supporting materials including backgrounders, infographics and images, please visit: https://www.astrazeneca.com/oncology-events where they are available throughout WCLC 2016.
About AURA3
AURA3 compared the efficacy and safety of Tagrisso<> 80mg once daily and platinum-based doublet chemotherapy (platinum-pemetrexed) in 419 patients with EGFR T790M mutation-positive, locally-advanced or metastatic NSCLC whose disease had progressed on or after treatment with a previous EGFR tyrosine kinase inhibitor (TKI). The trial was carried out in more than 130 locations worldwide, including the USA, Canada, Europe, China, Japan, Korea and Australia.
The primary endpoint of the trial was PFS, and secondary endpoints included overall survival (OS), overall response rate (ORR), duration of response (DoR), disease control rate (DCR), safety and measures of health-related quality of life (HRQoL).
About Non-Small Cell Lung Cancer (NSCLC)
Lung cancer is the leading cause of cancer death among both men and women, accounting for about one-third of all cancer deaths and more than breast, prostate and colorectal cancers combined. Among patients with lung cancer, 25% to 40% have brain metastases at some time in the course of their disease. Patients who have the EGFRm form of NSCLC, which occurs in 10-15% of NSCLC patients in the US and Europe and 30-40% of NSCLC patients in Asia, are particularly sensitive to treatment with currently-available EGFR-TKIs, which block the cell signalling pathways that drive the growth of tumour cells. However, tumours almost always develop resistance to treatment, leading to disease progression. Approximately two-thirds of patients develop resistance to approved EGFR-TKIs such as gefitinib and erlotinib due to the secondary mutation, T790M.
About Tagrisso
Tagrisso (osimertinib, AZD9291) 80mg once daily tablet is approved in the US, EU, Japan, Canada, Switzerland, Israel, Mexico, Australia and a number of other countries as the first treatment for patients with locally-advanced or metastatic EGFR T790M mutation-positive NSCLC. Tagrisso is also approved in South Korea in the same indication. Eligibility for treatment with Tagrisso is dependent on confirmation that the EGFR T790M mutation is present in the tumour.
Tagrisso has one of the fastest development programmes, from start of clinical trials to approval in just over two and a half years. Tagrisso is as an irreversible EGFR inhibitor, born out of scientific exploration and engineered to combat the mechanism of resistance by targeting the T790M resistance mutation. Tagrisso is also investigated in the adjuvant and metastatic first-line settings, including in patients with and without brain metastases, in leptomeningeal disease, and in combination with other treatments.
About AstraZeneca in Oncology
AstraZeneca has a deep-rooted heritage in Oncology and offers a quickly growing portfolio of new medicines that has the potential to transform patients’ lives and the Company’s future. With at least six new medicines to be launched between 2014 and 2020, and a broad pipeline of small molecules and biologics in development, we are committed to advance New Oncology as one of AstraZeneca’s six Growth Platforms focused on lung, ovarian, breast and blood cancers. In addition to our core capabilities, we actively pursue innovative partnerships and investments that accelerate the delivery of our strategy as illustrated by our investment in Acerta Pharma in haematology.
By harnessing the power of four scientific platforms – immuno-oncology, the genetic drivers of cancer and resistance, DNA damage response and antibody drug conjugates – and by championing the development of personalised combinations, AstraZeneca has the vision to redefine cancer treatment and one day eliminate cancer as a cause of death.
About AstraZeneca
AstraZeneca is a global, science-led biopharmaceutical company that focuses on the discovery, development and commercialisation of prescription medicines, primarily for the treatment of diseases in three main therapy areas - Oncology, Cardiovascular & Metabolic Diseases and Respiratory. The Company also is selectively active in the areas of autoimmunity, neuroscience and infection. AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. For more information, please visit www.astrazeneca.com and follow us on Twitter @AstraZeneca.
CONTACTS
Media Enquiries
|
|
|
Neil Burrows |
UK/Global |
+44 203 749 5637 |
Vanessa Rhodes |
UK/Global |
+44 203 749 5736 |
Karen Birmingham |
UK/Global |
+44 203 749 5634 |
Rob Skelding |
UK/Global |
+44 203 749 5821 |
Jacob Lund |
Sweden |
+46 8 553 260 20 |
Michele Meixell |
US |
+1 302 885 2677 |
|
|
|
Investor Enquiries |
|
|
Thomas Kudsk Larsen |
|
+44 203 749 5712 |
Craig Marks |
Finance, Fixed Income, M&A |
+44 7881 615 764 |
Henry Wheeler |
Oncology |
+44 203 749 5797 |
Mitchell Chan |
Oncology |
+1 240 477 3771 |
Lindsey Trickett |
Cardiovascular & Metabolic Diseases |
+1 240 543 7970 |
Nick Stone |
Respiratory |
+44 203 749 5716 |
Christer Gruvris |
Autoimmunity, neuroscience & infection |
+44 203 749 5711 |
US toll-Free |
|
+1 866 381 7277 |