29 January 2021 07:00 GMT
Data at WCLC highlight potential for both antibody drug conjugates as targeted treatments in this setting
New data from AstraZeneca and Daiichi Sankyo Company, Limited (hereafter, Daiichi Sankyo)’s datopotamab deruxtecan (Dato-DXd; DS-1062) and Enhertu (trastuzumab deruxtecan) showed encouraging results from both antibody drug conjugates (ADCs) in patients with advanced or metastatic non-small cell lung cancer (NSCLC). The data were presented today in two oral presentations during the World Conference on Lung Cancer (WCLC), hosted by the International Association for the Study of Lung Cancer (IASLC).
Updated results from the TROPION-PanTumor01 Phase I trial showed promising clinical activity for datopotamab deruxtecan, a TROP2-directed ADC, in patients with advanced or metastatic NSCLC.
Additionally, an interim analysis of the HER2-overexpressing cohort of the DESTINY-Lung01 Phase II trial showed preliminary evidence of antitumour activity for Enhertu, a HER2-directed ADC, in patients with metastatic NSCLC.
Lung cancer is the leading cause of cancer death among both men and women, and accounts for about one-fifth of all cancer deaths globally, with 80-85% classified as NSCLC.1-3 For patients with metastatic disease, prognosis is particularly poor, as only 6-10% live five years beyond diagnosis.4 Currently, there are no TROP2-directed or HER2-directed medicines approved for the treatment of NSCLC.
Cristian Massacesi, Senior Vice President, Head of Late-Stage Development, Oncology R&D, said: “Antibody drug conjugates have transformative potential for the targeted treatment of advanced lung cancer, and the early data for datopotamab deruxtecan and Enhertu suggest a promising durable benefit in patients who have limited treatment options. Both are potent ADCs, and we look forward to further clinical data from these development programmes in patients with lung cancer.”
Antoine Yver, Executive Vice President and Global Head, Oncology Research and Development, Daiichi Sankyo, said: “Developing innovative therapies for patients with lung cancer, including those that target TROP2 and HER2, are important as few treatment options remain once progression occurs in the metastatic setting following treatment with platinum-based chemotherapy and immune checkpoint inhibitors. We are encouraged by these preliminary results, which may indicate a durability of effect of datopotamab deruxtecan. We remain committed with AstraZeneca to our bold development plan, particularly the ongoing pivotal Phase III trial of datopotamab deruxtecan monotherapy in patients with metastatic non-small cell lung cancer.”
TROPION-PanTumor01 trial results
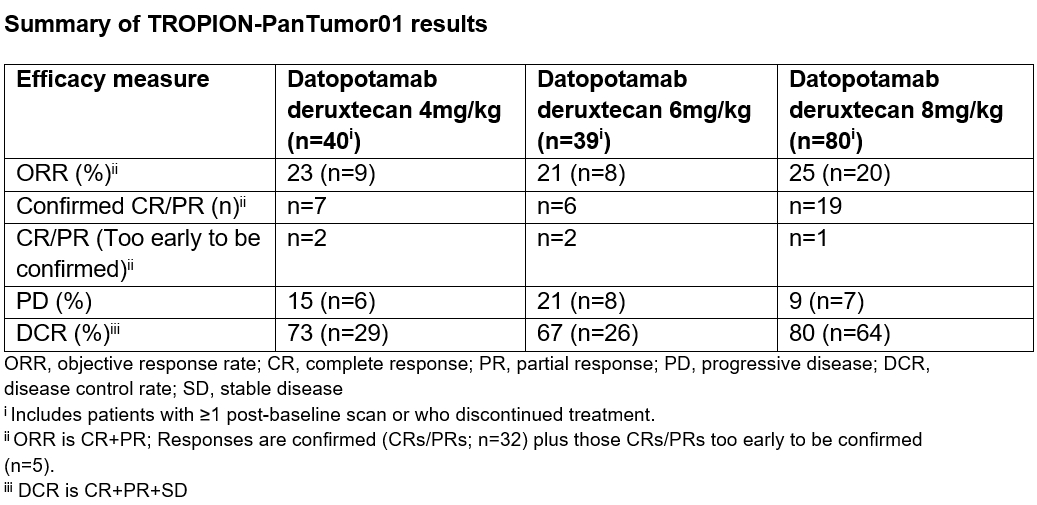
In the TROPION-PanTumor01 Phase I trial, an objective response rate (ORR) ranging from 21 to 25%, as assessed by independent central review, was observed in 159 patients with advanced or metastatic NSCLC receiving different doses of datopotamab deruxtecan (4mg/kg, 6mg/kg or 8mg/kg), as of data cut-off on 4 September 2020. Thirty two confirmed complete or partial responses were seen, and an additional five complete or partial responses are still too early to confirm. Efficacy data were preliminary due to immaturity of follow-up across dose groups, but preliminary efficacy results may support durability of clinical activity. A disease control rate (DCR) ranging from 67 to 80% was observed with a median progression-free survival (PFS) ranging from 4.3 to 8.2 months across the three doses of datopotamab deruxtecan.
Alexander Spira, MD, PhD, FACP, Oncologist, Virginia Cancer Specialists, US Oncology Research and Johns Hopkins Oncology, said: “These updated preliminary results from TROPION-PanTumor01 are encouraging, as responses were seen across all three doses of datopotamab deruxtecan, underscoring the potential of targeting TROP2 with an antibody drug conjugate in advanced or metastatic non-small cell lung cancer. We look forward to seeing the results from the Phase III trial, which will further evaluate datopotamab deruxtecan versus chemotherapy, the current standard of care for patients with advanced disease that has progressed following treatment with platinum chemotherapy and immunotherapy.”
The majority of patients across all three doses were previously treated with three or more prior lines of therapy including platinum-based chemotherapy (94%) or immunotherapy (84%). Median duration of follow-up was 7.4 months. As of data cut-off, 39% of patients remained on treatment with datopotamab deruxtecan.
Datopotamab deruxtecan demonstrated a manageable safety profile in the TROPION-PanTumor01 Phase I trial, which was consistent with what has been previously reported. Overall, the 4mg/kg and 6mg/kg doses were better tolerated than the 8mg/kg dose. The most common Grade 3 or greater treatment-emergent adverse events (TEAEs) included mucosal inflammation, anaemia, stomatitis and fatigue, with patients treated at the 8mg/kg dose experiencing higher rates overall. Fourteen cases (8%) of interstitial lung disease (ILD) occurred as determined by an independent adjudication committee. The majority of ILD cases (12/14) were observed with the 8mg/kg cohort, including three deaths (Grade 5). One Grade 3 ILD event was seen with the 4mg/kg dose and one Grade 2 ILD event was seen with the 6mg/kg dose.
Based on the efficacy and safety findings, the 6mg/kg dose has been identified as the recommended dose for the registrational TROPION-Lung01 Phase III trial.
DESTINY-Lung01 trial results
In the interim results of cohort 1 from the DESTINY-Lung01 Phase II trial the primary endpoint of confirmed ORR, assessed by independent central review, was 24.5% for extensively treated patients with HER2-overexpressing (defined as IHC3+ or IHC2+) metastatic NSCLC treated with Enhertu (6.4mg/kg) (n=49). Patients achieved a DCR of 69.4% with a median PFS of 5.4 months. After a median follow-up of 6.1 months, the estimated median duration of response (DoR) was 6.0 months, and the median overall survival (OS) was 11.3 months.
Patients were treated with a median of three prior lines of therapy with most receiving platinum-based chemotherapy (91.8%) or immunotherapy (73.5%). Median treatment duration was 18 weeks. As of data cut-off on 30 May 2020, 22% of patients remained on treatment with Enhertu.
Interim data (n=42) from the HER2-mutant (HER2m) metastatic NSCLC cohort of DESTINY-Lung01 were previously presented during the 2020 American Society of Clinical Oncology (ASCO) virtual meeting, and also featured as an encore presentation at WCLC. The results showed Enhertu achieved a clinically meaningful tumour response in patients with HER2m metastatic NSCLC.
The overall safety and tolerability profile of Enhertu was consistent with previous trials. In the HER2-overexpressing cohort of DESTINY-Lung01, the most common Grade 3 or greater TEAEs were decreased neutrophil count and fatigue. There were eight cases of treatment-related ILD or pneumonitis, as determined by an independent adjudication committee including two Grade 1, three Grade 2 and three deaths (Grade 5). In the HER2m cohort of DESTINY-Lung01, there were five cases of ILD or pneumonitis, as determined by an independent adjudication committee. All cases were Grade 2.
About NSCLC
Lung cancer is the leading cause of cancer death among both men and women and accounts for about one-fifth of all cancer deaths.1 NSCLC accounts for approximately 80-85% of all lung cancers. 2,3 For patients with metastatic disease, prognosis is particularly poor, as only 6-10% live five years beyond diagnosis.4 The introduction of targeted therapies and checkpoint inhibitors in recent years has improved the treatment landscape for patients with advanced NSCLC; however, new approaches are needed for those who are not eligible for available treatments, or whose cancer continues to progress.5 Currently, there are no TROP2-directed or HER2-directed medicines approved for the treatment of NSCLC.
TROP2 (trophoblast cell-surface antigen 2) is a transmembrane glycoprotein that is overexpressed in many cancers.6 TROP2 expression has been associated with poor overall and disease-free survival in several types of solid tumours. TROP2 expression has been observed in up to 64% of adenocarcinoma and up to 75% of squamous cell carcinoma NSCLC.7-9
HER2 is a tyrosine kinase receptor growth-promoting protein expressed on the surface of many types of tumours, including lung, breast, gastric and colorectal cancers. HER2 overexpression is associated with a specific HER2 gene alteration known as HER2 amplification and is often associated with aggressive disease and poorer prognosis. It has been reported in up to one third of patients with NSCLC.10-12
Other HER2 gene alterations (called HER2 mutations) have been identified in NSCLC, specifically adenocarcinomas, as distinct molecular targets and have been reported in approximately 2-4% of patients with NSCLC.11,13-15 These acquired HER2 gene mutations have been independently associated with cancer cell growth and poor prognosis.13,14
About TROPION-PanTumor01
TROPION-PanTumor01 is a first-in-human, open-label, two-part, multicentre Phase I trial designed to evaluate the safety, tolerability and preliminary efficacy of datopotamab deruxtecan in patients with advanced solid tumours, including NSCLC and triple-negative breast cancer (TNBC), that are refractory to or relapsed from standard treatment — or for whom no standard treatment is available.
The first part of the trial (dose escalation) assessed the safety and tolerability of increasing doses of datopotamab deruxtecan to determine the maximum tolerated dose and/or recommended dose for expansion in patients with unresectable advanced NSCLC. The second part of the trial (dose expansion) is further assessing the safety and tolerability of datopotamab deruxtecan at selected dose levels (4mg/kg, 6mg/kg and 8mg/kg) in patients with NSCLC, and in patients with unresectable/advanced or metastatic TNBC.
Safety endpoints include dose-limiting toxicities and serious adverse events. Efficacy endpoints include ORR, DoR, DCR, time to response, PFS and OS. Pharmacokinetic, biomarker and immunogenicity endpoints also are being evaluated.16
About DESTINY-Lung01
DESTINY-Lung01 is a global, Phase II, open-label, multicentre, two-cohort trial evaluating the safety and efficacy of Enhertu in 170 patients with HER2m (6.4mg/kg) or HER2- overexpressing (defined as IHC3+ or IHC2+; 6.4mg/kg and 5.4mg/kg) unresectable and metastatic non-squamous NSCLC. Patients had progressed after one or more systemic therapies including chemotherapy, molecular targeted therapy or immunotherapy. The primary endpoint is ORR by independent central review. Key secondary endpoints include DoR, DCR, PFS and OS.17
Daiichi Sankyo Collaboration
Enhertu (trastuzumab deruxtecan; fam-trastuzumab deruxtecan-nxki in the US only) and datopotamab deruxtecan (Dato-DXd; DS-1062) are two lead DXd ADCs in the oncology pipeline of Daiichi Sankyo, and the most advanced programmes in AstraZeneca’s ADC scientific platform.
Each ADC is engineered using Daiichi Sankyo’s proprietary and portable DXd ADC technology to target and deliver chemotherapy inside cancer cells that express a specific cell surface antigen. Both Enhertu (a HER2-directed ADC) and datopotamab deruxtecan (a TROP2-directed ADC) consist of a monoclonal antibody attached to a topoisomerase I inhibitor payload, an exatecan derivative, via a stable tetrapeptide-based cleavable linker.
AstraZeneca and Daiichi Sankyo entered into a global collaboration to jointly develop and commercialise Enhertu in March 2019, and datopotamab deruxtecan in July 2020, except in Japan where Daiichi Sankyo maintains exclusive rights. Daiichi Sankyo is responsible for manufacturing and supply of Enhertu and datopotamab deruxtecan.
AstraZeneca in lung cancer
AstraZeneca has a comprehensive portfolio of approved and potential new medicines in late-stage development for the treatment of different forms of lung cancer spanning different histologies, several stages of disease, lines of therapy and modes of action.
AstraZeneca aims to address the unmet needs of patients with EGFRm tumours as a genetic driver of disease, which occur in 10-15% of NSCLC patients in the US and EU and 30-40% of NSCLC patients in Asia, with the approved medicines Iressa (gefitinib) and Tagrisso and its ongoing LAURA, NeoADAURA and FLAURA2 Phase III trials. AstraZeneca is committed to addressing tumour mechanisms of resistance through the ongoing SAVANNAH and ORCHARD Phase II trials, which test Tagrisso in combination with savolitinib, a selective inhibitor of c-MET receptor tyrosine kinase, along with other potential new medicines.
The Company is also evaluating the potential of ADCs to improve patient outcomes in NSCLC. Enhertu is in development for metastatic non-squamous HER2-overexpressing or HER2m NSCLC including trials in combination with other anticancer treatments. In addition, datopotamab deruxtecan is in early development for advanced NSCLC where TROP2 is overexpressed in the majority of tumours.
An extensive Immuno-Oncology development programme focuses on lung cancer patients without a targetable genetic mutation, which represent up to three quarters of all patients with lung cancer. Imfinzi, an anti-PDL1 antibody, is in development for patients with advanced disease (POSEIDON and PEARL Phase III trials) and for patients in earlier stages of disease, including potentially curative settings (MERMAID-1, MERMAID-2, AEGEAN, ADJUVANT BR.31, PACIFIC-2, PACIFIC-4, PACIFIC-5, and ADRIATIC Phase III trials) both as monotherapy and in combination with tremelimumab and/or chemotherapy. Imfinzi is also in development in the NeoCOAST, COAST and HUDSON Phase II trials in combination with potential new medicines from the early-stage pipeline, including Enhertu.
AstraZeneca in oncology
AstraZeneca has a deep-rooted heritage in oncology and offers a quickly growing portfolio of new medicines that has the potential to transform patients’ lives and the Company’s future. With seven new medicines launched between 2014 and 2020, and a broad pipeline of small molecules and biologics in development, the Company is committed to advance oncology as a key growth driver for AstraZeneca focused on lung, ovarian, breast and blood cancers.
By harnessing the power of six scientific platforms – Immuno-Oncology, Tumour Drivers and Resistance, DNA Damage Response, Antibody Drug Conjugates, Epigenetics, and Cell Therapies – and by championing the development of personalised combinations, AstraZeneca has the vision to redefine cancer treatment and, one day, eliminate cancer as a cause of death.
AstraZeneca
AstraZeneca (LSE/STO/Nasdaq: AZN) is a global, science-led biopharmaceutical company that focuses on the discovery, development and commercialisation of prescription medicines, primarily for the treatment of diseases in three therapy areas - Oncology, Cardiovascular, Renal & Metabolism, and Respiratory & Immunology. Based in Cambridge, UK, AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. Please visit astrazeneca.com and follow the Company on Twitter @AstraZeneca.
Contacts
For details on how to contact the Investor Relations Team, please click here. For Media contacts, click here.
References
1. World Health Organization. International Agency for Research on Cancer. Lung Fact Sheet. Available at: http://gco.iarc.fr/today/data/factsheets/cancers/15-Lung-fact-sheet.pdf. Accessed January 2021.
2. ASCO. Cancer.net. Lung cancer – non-small cell. Available at: https://www.cancer.net/cancer-types/lung-cancer/view-all. Accessed January 2021.
3. Cheema PK, et al. Perspectives on treatment advances for stage III locally advanced unresectable non-small-cell lung cancer. Curr Oncol. 2019;26(1):37-42.
4. Goldstraw P, et al. The IASLC Lung Cancer Staging Project: proposals for revision of the TNM Stage Groupings in the forthcoming (eighth) edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39-51.
5. Economopoulou P, et al. The emerging treatment landscape of advanced non-small cell lung cancer Ann Transl Med. 2018;6(8):138.
6. Inamura K, et al. Association of tumor TROP2 expression with prognosis varies among lung cancer subtypes. Oncotarget. 2017;8(17):28725-28735.
7. Pak M, et al. Significance of EpCAM and TROP2 expression in non-small cell lung cancer. World J Surg Oncol. 2012;10:53.
8. Li Z, et al. TROP2 overexpression promotes proliferation and invasion of lung adenocarcinoma cells. Biochem Biophys Res Commun. 2016;470:197-204.
9. Liu T, et al. Overexpression of TROP2 predicts poor prognosis of patients with cervical cancer and promotes the proliferation and invasion of cervical cancer cells by regulating ERK signaling pathway. PLoS One. 2013;8:e75864.
10. Hirsch FR, et al. Lung cancer: current therapies and new targeted treatments. Lancet Long Engl. 2017;389:299-311.
11. Pillai RN, et al. HER2 mutations in lung adenocarcinomas: a report from the Lung Cancer Mutation Consortium. Cancer. 2017;123(21):4099-4105.
12. The National Comprehensive Care Network (NCCN). NCCN Clinical Practice Guidelines in Non-Small Cell Lung Cancer Version 3. 2020.
13. Liu S, et al. Targeting HER2 Aberrations in Non-Small Cell Lung Cancer with Osimertinib. Clin Cancer Res. 2018;24(11):2594-2604.
14. Campbell JD, et al. Distinct patterns of somatic genome alterations in lung adenocarcinomas and squamous cell carcinomas. Nat Genet. 2016 Jun;48(6):607-16.
15. Li BT, et al. HER2 amplification and HER2 mutation are distinct molecular targets in lung cancers. J Thorac Oncol. 11(3):414-9.
16. Clinicaltrials.gov. First-in-human study of DS-1062a for advanced solid tumors. Available at: https://clinicaltrials.gov/ct2/show/NCT03401385. Accessed January 2021.
17. Clinicaltrials.gov. DS-8201a in human epidermal growth factor receptor 2 (HER2)-expressing or -mutated non-small cell lung cancer (DESTINY-Lung01). Available at: https://clinicaltrials.gov/ct2/show/NCT03505710. Accessed January 2021.