
Systemic lupus erythematosus
Home / Our therapy areas / Respiratory & Immunology / Lupus
We are a disruptor in Immunology
Our ambition is to bring forth new transformational therapies for multiple immune-mediated diseases. We aim to move beyond symptom control to drive clinical remission and, eventually, cure in immune-mediated diseases with high unmet need, such as systemic lupus erythematosus (SLE).
We intend to show the world what science can do... as we strive to transform outcomes for those living with immune-mediated diseases.
What is systemic lupus erythematosus?
SLE is a chronic disease in which the body’s immune system attacks healthy tissue in any part of the body.1 It’s experienced differently by each person and can cause a wide range of debilitating symptoms, including skin rash, joint pain, swelling and fevers.2 There have been very few new medicines for SLE, and the significant physical, emotional and socio-economic burden remains high for people living with the disease.3,4
Unlocking the science of systemic lupus erythematosus
In people living with SLE, their immune system dysfunctions and inappropriately attacks healthy tissue within the body.1 SLE disease activity involves B, T and dendritic cells, as well as inflammatory cytokines such as type 1 interferons (IFN-1), IL-6 and B-cell activating factor.5 Cytokines are molecules that act as immune signallers, regulating processes along immune pathways that coordinate the overall immune response.5 Normally, these cells come together to act as a defence network that protects us from infection.6 In SLE, this dysfunction results in the immune system attacking tissues in the body.6 This can lead to inflammation, and in some cases permanent tissue damage, which can be widespread, affecting the skin, joints, heart, lung kidneys, blood cells and brain.7 Up to 60-80% of adults with SLE have an elevated IFN-1 gene signature, which can be associated with increased disease severity.8,9
By understanding the role key cytokines play in the inflammatory cascade, we can begin to further unlock the complex nature of this challenging disease.
Scientists at AstraZeneca are building on existing disease knowledge and emerging biology, applying learnings from other therapeutic areas, such as cancer, to advance new treatment approaches for SLE. These efforts are critical for those people with SLE who continue to experience inadequate disease control with current therapies. Advanced modalities, such as novel antibody approaches and cell therapies, are being explored to help control the underlying processes that cause SLE with the goal of achieving lasting disease remission.
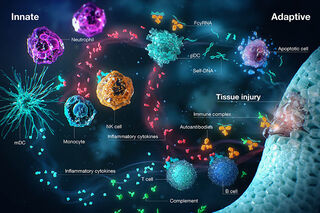
The biological mechanism behind SLE. Dysregulation in the innate immune system and adaptive immune responses results in chronic autoimmune conditions and disease progression.9
The burden of systemic lupus erythematosus
Over 3.4 million people worldwide are affected by SLE.10 The chronic and complex disease is known as ‘the great imitator’ because its symptoms mimic many other illnesses, and it can take up to six years for a patient to be diagnosed after first experiencing symptoms.11,12
90% of people with lupus are women. The disease disproportionately affects those of African American, Asian or Hispanic ethnicities.12
Mortality can be up to 5 times higher in younger patients (<45 years) and 3 times higher in women, compared to the general population.13,14,15,16
Lupus places a significant financial burden, driven by inpatient costs, on patients, their families and health systems.17,18
In addition to physical symptoms, lupus can reduce quality of life for patients, and can cause mood disorders, and feelings of depression and anxiety.17
Addressing unmet needs in the lupus community
SLE is a remitting and relapsing disorder (meaning symptoms come and go) characterised by unpredictable flares of worsening pain and inflammation.4,19,20 Even with treatment many patients with lupus may face permanent organ damage, uncontrolled disease activity and even death.1
Patients often rely on prolonged use of treatments, such as oral corticosteroids (OCS) that offer some relief from symptoms but do not target the underlying drivers of lupus.21 OCS are used by approximately 80% of people with SLE to control flares, yet OCS use contributes to irreversible organ damage.22 As a result, many have an inadequate treatment response and few experience remission.21 Data show that reducing OCS use may reduce organ damage and healthcare costs, and that achieving remission is associated with improved prognosis, mortality and health-related quality of life.23
Recent recommendations by the European Alliance of Associations for Rheumatology (EULAR) advocate aiming for a treatment target of remission or low disease activity to reduce the risk of organ damage and adverse outcomes in patients. To achieve these goals EULAR advises clinicians take an OCS-sparing approach to treatment.24
There is an urgent need to improve patient outcomes and address the unmet medical needs associated with the condition.

Our ambition in lupus: making remission a reality
EULAR defines remission in SLE according to the Definition of Remission in SLE (DORIS) criteria, as having no disease activity while receiving treatment of antimalarials, immunosuppressives or biologics, but low dose or no OCS.24,25
We’re unlocking the science of the immune system to address the significant unmet needs in lupus. By investigating the underlying drivers of this complex disease we aim to bring scientific advancements to the lupus community – including remission – and challenge boundaries that have been accepted for too long.

Our ambition is to disrupt Immunology by achieving increased rates of remission in under-served diseases like lupus. We want to bring in a new generation of therapeutics, aiming to reverse and repair damage, treat patients earlier, modify the course of disease, and one day offer a cure.
Living with lupus
Lupus affects each person differently and can be unpredictable. Hear from people with SLE on how the disease has impacted their lives since diagnosis, and their hope for scientific advancements in the field.
Ingrid

US
Living with lupus
I was diagnosed with lupus when I was 23 and have been a Lupus Warrior for 17 years. At different points in my life, I have experienced various symptoms, including skin rash, joint pain and extreme fatigue, in addition to the emotional journey that’s attached to the condition. At times these can be debilitating and it’s like a rollercoaster. There’s highs, there’s lows. But I’m more hopeful today than ever that scientific progress is being made to help improve the lives of people like me who are living with lupus.
Jule

Germany
Living with lupus
I was diagnosed with lupus in 2018 when I was 19. Over the last few years, I’ve experienced severe pain in my joins and connective tissues and suffered hair loss and excessive sweating. There are days when I can hardly move; there are days when I’m sad or angry, but I’ve come to accept my disease. Still, it’s important to continue raising awareness of lupus and the different treatment options. I want others living with lupus to remain hopeful for the future and remember that lupus lives with you, you do not live with lupus.
Jeanette

Denmark
Living with lupus
I was diagnosed with lupus in 2011, whilst on my honeymoon. The diagnosis forced me to reassess my career aspirations and give up my dream of enrolling in a PhD placement. Whilst the diagnosis has changed the course of my life, I have taken my love of learning to understand lupus as a disease and build a better future in lupus care. Ensuring that lupus patients have access to the healthcare professionals they need, as well as knowledge of and access to the care options best suited to them, is a key advocacy goal, and I have never done anything that makes as much sense as what I am doing now.
Heidi

Canada
Living with lupus
I was diagnosed with lupus at the age of 21. Living with lupus is unique to everyone. For me, I had a skin rash, arthritis and kidney scarring. The thing I have learned the most is to be your own advocate. I think it’s important to keep looking for the answers that you want, because I believe living well with lupus is possible.
Anne-Sophie

France
Living with lupus
I was diagnosed seven years ago, in 2017. The first time the doctor explained what lupus was to me, it was quite vague, and I didn’t really understand the challenges I was about to face. Lupus can affect several organs, and in my case, lupus mainly affects my joints, so I have chronic pain in my shoulders, elbows, knees and ankles. For a long time, I hid my lupus because I was ashamed of it, I didn’t want people to find out and I didn’t want to talk about it. I’ve had to adapt my life to live with this disability and rethink my plans. However, my message of hope is to never give up, even when you feel alone. The psychological aspect plans a decisive role in the frequency of relapses. You need to be able to set yourself goals so you don’t sink, and above all, you need to be well surrounded so you don’t isolate yourself.
Looking to the future
Although clinical research in Immunology is fast-growing, there remains a high unmet need for many people living with immune-mediated diseases.26 As a disruptor in Immunology, we aspire to help patients with immune-mediated diseases move beyond symptom control to achieve remission, and one day, cure. We are investigating pathways in other immune-mediated diseases such as Crohn’s disease, myositis, systemic sclerosis and eosinophilic granulomatosis with polyangiitis (EGPA) to deepen our understanding of their drivers.
You may also like

References
- Bruce IN, et al. Factors associated with damage accrual in patients with systemic lupus erythematosus: results from the systemic lupus international collaborating Clinics (SLICC) inception cohort. Ann Rheum Dis. 2015;74:1706-1713.
- American College of Rheumatology. Guidelines for referral and management of systemic lupus erythematosus in adults. Arthritis Rheumatol. 1999;42:1785-1796.
- Mahieu MA, et al. A critical review of clinical trials in systemic lupus eythematosus. Lupus. 2016; 25 (10): 1122-1140.
- Merrill JT, et al. Lupus community panel proposals for optimising clinical trials: 2018. Lupus Sci Med. 2018;5:E000258.
- Ameer MA, et al. An overview of systemic lupus erythematosus (SLE) pathogenesis, classification, and Management. Cureus. 2022;14(10):e30330.
- Lupus UK. The Immune System and Lupus. Available at: https://lupusuk.org.uk/medical/lupus-diagnosis-treatment/introduction-to-lupus/the-immune-system/ [Last accessed April 2024].
- Becker AM, et al. SLE peripheral blood B cell, T cell and myeloid cell transcriptomes display unique profiles and each subset contributes to the interferon signature. PLoS One. 2013;8(6):e67003.
- Crow MK. Type I interferon in the pathogenesis of lupus. J Immunol. 2014;192(12):5459-5468.
- Jefferies CA. Regulating IRFs in IFN driven disease. Front Immunol. 2019;10:325.
- Tian J, et al. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study.Ann Rheum Dis. 2023;82:351-356.
- Sloan M, et al. Medically explained symptoms: a mixed methods study of diagnostic, symptom and support experiences of patients with lupus and related systemic autoimmune diseases. Rheumatol Adv Pract. 2020;4(1).
- Lupus Foundation of America. Lupus facts and statistics. Available at: https://www.lupus.org/resources/lupus-facts-and-statistics [Last accessed April 2024].
- Lee YH, Choi SJ and Song GG. Overall and cause-specific mortality in systemic lupus erythematosus: an updated meta-analysis. Lupus. 2016;25:727–734.
- Zen M, et al. Mortality and causes of death in systemic lupus erythematosus over the last decade: Data from a large population-based study. Eur J Int Med. 2023:45-51.
- Frances Rees, et al. Mortality in systemic lupus erythematosus in the United Kingdom 1999–2012, Rheumatology, 2016;55:854-860
- Chunhuan Lao, et al, Mortality and causes of death in systemic lupus erythematosus in New Zealand: a population-based study, Rheumatology, 2023;, kead427.
- Olesińska M, Saletra A. Quality of life in systemic lupus erythematosus and its measurement. Reumatologia. 2018;56(1):45-54. Epub 2018. PMID: 29686443.
- Jiang M, et al. Frequency, Severity and Costs of Flares Increase with Disease Severity in Newly Diagnosed Systematic Lupus Erythematous: A Real-World Cohort Study, United States 2004-2015. American College of Rheumatology Annual Meeting; 2019.
- Lupus Foundation of America. Common symptoms of lupus. Available at: https://www.lupus.org/resources/common-symptoms-of-lupus [last accessed April 2024].
- Lupus Foundation of America. Facts and statistics. Available at: https://www.lupus.org/resources/lupus-facts-and-statistics [last accessed April 2024].
- Fanouriakis A, et al. Changing paradigms in the treatment of systemic lupus erythematosus. Lupus Science & Medicine. 2019; 6: e000310.
- Apostolopoulos, D. and Morand, F., It hasn't gone away: the problem of glucocorticoid use in lupus remains. Rheumatology. 2017; 56: 114-122, p.2.
- Kabadi S, et al. Healthcare resource utilization and costs associated with long-term corticosteroid exposure in patients with systemic lupus erythematosus. Lupus. 2018;27(11):1799-1809.
- Fanouriakis A, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases 2024.
- Van Vollenhoven RF, et al. 2021 doris definition of remission in SLE: Final recommendations from an International Task Force. Lupus Science & Medicine. 2022;9(1).
- Touma Z, et al. Current and future therapies for SLE: obstacles and recommendations for the development of novel treatments. Lupus Sci Med. 2017;4: e000239.