This year’s International NASH Day represents a global effort to raise visibility and urgency around non-alcoholic steatohepatitis (NASH) and focuses on how people can take action to address the life-threatening consequences of this liver disease. We share the same mission, taking action to develop groundbreaking R&D approaches to slow or stop disease progression.
Driving NASH diagnosis earlier in disease to improve patient outcomes
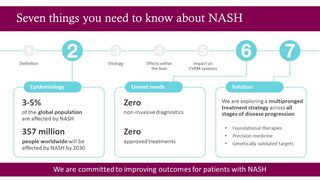
Despite its growing prevalence, NASH is frequently underdiagnosed, and patients may not be identified until they develop symptoms from late-stage complications.1 The disease has a gradual onset ‒ over years to decades ‒ and the early stages are often clinically silent and overlooked by both patients and clinicians.2 This, combined with a lack of precise non-invasive diagnostics, often leads to late, or even missed diagnoses.3,4
As we progress our NASH therapies into late-stage clinical development, there is a fast-growing need for large-scale recruitment of patients with NASH. Yet, due to the difficulties in diagnosing, identifying and engaging patients with NASH, there is a lack of candidates eligible for clinical trials. In precision medicine research, these trials target specific genetically defined populations, making it necessary to screen many more patients to identify those with the relevant characteristics. Here, we are transforming how we identify patients with the highest risk of developing NASH by genetically testing participants to support our precision medicine programmes. In addition, we are developing ways to simplify how our clinical trials operate, making participation easier for clinicians and patients with NASH.
We are also ensuring doctors have all the information they need to recommend the right participants for trials. Educating healthcare professionals, particularly those who are exposed to patients in high-risk settings such as diabetes and obesity, is essential to identifying suitable participants for clinical trials.
Our goal is to bring life-changing NASH treatments to patients sooner. That means understanding and addressing the high unmet needs for diagnosis and disease awareness by innovating across the entire drug development process, including the critical stages of clinical trial recruitment. Today, recruitment rates remain low, and the present system cannot adequately support the 130+ NASH clinical trials that are underway.5 We need to take this opportunity to adapt our approach to conventional clinical trials and bring therapies to patients sooner.
Discover more about NASH and how it relates to our overall metabolic health from Dr Arun Sanyal, Professor of Medicine, Virginia Commonwealth University

In the following sections we’ll talk about some of the key actions we’re taking to transform clinical development for patients with NASH.
Accelerate clinical trial recruitment
We are at the forefront of clinical trial innovation, highly focused on improving and simplifying the recruitment process and benefits to physicians and patients including:
- Giving more patients with NASH the opportunity to choose between multiple suitable interventional NASH clinical trials, so they can take part and personally select those trials most relevant or convenient to them.
- Closely linking a network of genetic pre-screening sites to our collection of interventional trials, enabling rapid assessment of trial eligibility based on the characteristics of their illness, including genetic drivers and disease stage.
- Providing a single point of care for education, screening, and trial interventions with the potential to receive enhanced access to targeted treatments based on genetic insight and risk profile.
- The opportunity for trial sites to participate in multiple interventional trials, where they can be more active partners. Sites will also benefit from a model tailored to their specific needs and processes.
- Improving workflows between sites and our teams, helping build collaborative relationships at the start of the journey and enabling global teams use local insights to adapt trial processes and protocols.
This approach to trial delivery is great because it enables us to do more for many patients living with NASH before they progress to late-stage illness.
Looking beyond this initiative, the development of a more accessible and affordable test as a less invasive alternative to liver biopsy would enable more at-risk patients to be screened. To that end, we have partnered with research consortia, such as LITMUS in Europe and NIMBLE in the US, to find potential non-invasive biomarkers for NASH that could be developed into new diagnostic tests.
Target key disease drivers
Following the science of NASH has helped us to find new ways to target the underlying causes in different populations. By integrating genetic testing into our screening process, we may be able to identify groups of patients with NASH that are most likely to benefit from specific precision medicine treatments. Such an approach will help to ensure that the right patients are recruited into the right trials based on the characteristics of their illness.
Tackling another important step in the development process, we’re developing sophisticated liver organoids to mimic NASH progression. Our ambition is to identify novel targets against which we can screen potential medicines and develop cell lines suitable for tissue regeneration in the liver.
Draw on our expertise across CVRM to combat NASH
The burden for NASH is set to increase significantly in parallel with increasing rates of obesity, and contributions from metabolic disease including diabetes and insulin resistance.1 At advanced stages, patients with NASH have an increased risk of developing hepatocellular carcinoma (HCC), the most common type of liver cancer.6 The incidence of NASH-induced cirrhosis is also expected to double over the next seven years,7 and the disease is now the fastest growing indication for liver transplant worldwide.8
However, the treatment of NASH has implications beyond the liver, and effective treatments could also address related co-morbidities. The interconnection of CVRM diseases is well established,9-11 and any new treatment for NASH may have a positive impact on the health of other organs, such as the heart and kidneys. We are proud of the action we are taking every day to improve outcomes for the millions of patients who are living with the complexities of CVRM diseases.12