Dyslipidaemia is characterised by elevated lipid and lipoprotein levels in the blood, particularly LDL-cholesterol (also known as ‘bad cholesterol’). High levels of LDL-C can drastically increase the risk of adverse cardiovascular (CV) outcomes such as coronary artery disease, stroke and heart failure.1-3 It is estimated that dyslipidaemia causes 2.6 million deaths worldwide,2,4 and the global burden of disease has been on the rise5
The growing burden of dyslipidemia
Dyslipidemia, or a dysregulation in the levels of circulating lipids in plasma, is a modifiable risk factor for cardiovascular disease and strongly associated with poor patient outcomes including stroke and myocardial infarction (MI). Of the many manifestations of dyslipidemia, hypercholesterolaemia is the most common form, with elevated plasma LDL-cholesterol (LDL-C) levels going from being the 15th leading risk factor for death in 1990, to 11th in 2007, and rising to 8th in 2019.
Management of dyslipidemia through LDL-C lowering therapies has demonstrated improvement in global outcomes from cardiovascular disease, both in primary prevention, which is to prevent or delay the onset of cardiovascular disease, and secondary prevention in patients with known cardiovascular disease to reduce risk of serious cardiovascular events.
The mainstay of cholesterol lowering: Inhibiting cholesterol synthesis with statins
One of the first targets for improving CV outcomes is elevated low-density lipoprotein cholesterol (LDL-C),6,7 due to its established role in increased CV risk.1,5 The current standard of care (SoC) for elevated LDL-C levels consists a number of lipid-lowering agents, including statins, which are widely used, effective, and generally well tolerated.8
Despite widespread use of lipid-lowering therapies, up to 70% of patients do not reach their LDL-C targets under the current SoC.7,9,10 This is due to issues like poor adherence and single-drug therapy often not being effective enough. Even among patients who meet LDL-C goals with the current SoC, 40% still experience life threatening CV events, indicating residual risk remains even when low LDL-C levels are achieved. Therefore, the current SoC may not be enough or suitable for every patient.7
The current step-up approach in the use of lipid-lowering therapies is complex and real-world adherence to a treatment schedule is hard to implement for patients and physicians. Being able to optimise treatment schedules which do not require repeated dose changes with combination strategies that work across multiple modes of action to reduce LDL cholesterol levels could potentially help improve outcomes for many more patients.
Addressing complementary mechanisms: The potential of statins and PSCK9 inhibition
There are two well-understood and validated pathways in cholesterol metabolism that have been identified as targets for reducing LDL-C levels: intracellular cholesterol synthesis and LDL-receptor (LDL-R) degradation.8,11 Statins reduce intracellular LDL-C levels by inhibiting a key enzyme involved in cholesterol synthesis.8 While statins address one of the two modes of action involved in LDL-C regulation, their efficacy can vary,10 suggesting that statins alone may be insufficient to lower LDL-C levels to target levels in some patients.7
In addition to statin-targeted intracellular LDL-C synthesis, the process of LDL-R recycling and degradation by the protein, PCSK9 (proprotein convertase subtilisin/kexin type 9) is another well-validated mechanism that can be targeted to lower LDL-C levels8,11,12
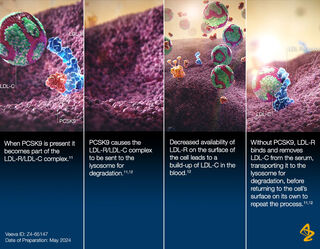
PCSK9 causes the LDLC/LDLR complex to be sent to the lysosome for degradation.11 By inhibiting PCSK9, the natural process of LDL-C removal from the bloodstream for lysosomal degradation is enhanced by increased LDL-R on the cell surface.11,12
Statins work to reduce total LDL-C levels by inhibiting intracellular LDL-C synthesis, while inhibition of PCSK9 can reduce LDL-C levels by increasing LDL-C clearance.8,11,12 Statins also indirectly increase expression of LDL-R and PCSK9, further increasing the amount of LDL-R on cell surfaces and potential LDL-C clearance.8,13 These two potentially complementary LDL-C-lowering effects of statins and PCSK9 inhibition offer the possibility of addressing multiple routes to reach lower LDL-C targets.7
Large, injectable biologicals such as monoclonal antibodies are known to be effective at inhibiting PCSK9, but the development of a small molecule PCSK9 inhibitor for oral use has proven to be more complex.14 This is because the site where PCSK9 interacts with LDL-R has been shown to be relatively large and flat, making small molecule design especially difficult.15
Future directions
While the current evidence demonstrates positive shifts in cardiovascular morbidity and mortality with LDL-lowering therapies, there is a need for innovation and optimising treatment options for dyslipidaemia to be able to tackle the growing number of patients including those with comorbidities such as diabetes, hypertension and obesity, which could put them at greater risk of developing CV disease.
Over the past few decades, we have advanced our understanding and recognition of high LDL-cholesterol as a modifiable risk factor in cardiovascular disease. However, we need to continue innovating in this space to be able to improve outcomes in patients who are not meeting their LDL-cholesterol targets and who remain at risk of a major cardiovascular event.
At AstraZeneca, we are deepening our understanding of the interconnections between risk factors such as dyslipidaemia and cardiovascular diseases to help develop a new wave of solutions. We are pioneering novel ways to target well-known disease pathophysiology and taking a patient-centric approach to build upon the current SoC to address residual risk. Where current therapies have their limitations, we want to address these barriers and be able to meet the needs of patients who are not attaining guideline-directed LDL-C target levels and remain at risk of CV disease.


