Written by:

Senior Global Medical Affairs Lead (CVRM), AstraZeneca

Executive Medical Director, AstraZeneca
What is aldosterone?
The renin-angiotensin-aldosterone system (RAAS) helps regulate blood pressure, electrolyte balance, and fluid volume in the body, making it integral to homeostasis.1-5 Dysregulation of this critical physiological feedback loop, particularly the upregulation of aldosterone, a mineralocorticoid steroid hormone, can contribute to hypertension, heart failure, and kidney disease.6 A deeper understanding of the mechanisms within this system may help uncover novel approaches to slowing disease progression.
The RAAS pathway and aldosterone production

The kidneys release renin in response to various stimuli, including low blood pressure (as detected by baroreceptors), decreased blood volume, and sympathetic nervous system activation, otherwise known as “fight or flight.”5,7 Functioning as an enzyme, renin catalyses the production of angiotensin I, which is then converted into angiotensin II, a vasoconstrictor that reduces the diameter of blood vessels, leading to increased blood pressure. 5
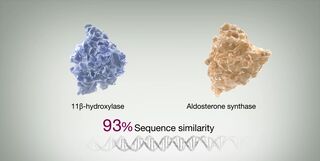
Angiotensin II also stimulates the adrenal glands to release aldosterone.2,3,5,8,9 Notably, the enzyme that catalyses the production of aldosterone, aldosterone synthase, shares a similar shape with 11β-hydroxylase, which is responsible for the production of cortisol.9-11 This structural similarity has made it difficult to develop a cortisol sparing therapy, i.e., one that selectively suppresses aldosterone, but not cortisol production.
Aldosterone and antidiuretic hormone (ADH) close the feedback loop of the RAAS pathway by causing the kidneys to reabsorb sodium and fluid, promoting potassium excretion into urine, and adjusting pH balance.2,5 Essentially, the kidneys sense the increased sodium concentration in the bloodstream and signal to “ease off the gas” with renin production. Other hormones and corticosteroids separate from the RAAS pathway, including oestrogen and thyroid hormones, can also trigger aldosterone synthesis.2,5 Any dysregulation in the RAAS pathway or these hormonal processes could lead to inappropriate aldosterone production.2
Inappropriately elevated aldosterone
Aldosterone helps regulate blood pressure, acting as a sensor for fluid homeostasis, and maintains blood pH balance by regulating sodium and potassium.2-5 Elevated aldosterone levels can be beneficial when salt intake is low or during excessive sweating.12,13 Of note, the current global mean intake of sodium is 4310 mg/d for adults, more than double the recommended sodium intake of 2000 mg/d.14
There are a number of conditions that can lead to inappropriately elevated levels of aldosterone:
- Primary aldosteronism, also known as Conn’s syndrome, which is when the adrenal glands produce too much aldosterone. Primary aldosteronism can be caused by adrenal adenomas, adrenal hyperplasia, or familial hyperaldosteronism type 1.15
- Secondary aldosteronism, which can occur if blood flow to the kidneys is reduced, either due to obstructive renal artery disease or conditions such as heart failure, which will then inappropriately trigger the RAAS pathway.15
- In high sodium concentrations, elevated aldosterone levels can cause hypertension (high blood pressure), a risk factor for cardiovascular disease and cardiorenal complications that are independent of the effects on blood pressure.6,16
In other words, for the same blood pressure levels, patients with excess aldosterone have a higher risk of adverse cardiorenal outcomes than patients without elevation of aldosterone (or elevated aldosterone that is appropriate for their sodium status).6,16,17 Studies indicate that there is a high prevalence of aldosteronism among patients with hypertension, particularly in those who have more severe or resistant hypertension.18
Aldosterone dysregulation occurs as a gradual, continuous process rather than an on/off switch from normal function to dysregulation.19 When inappropriately regulated, the normal feedback loop breaks down so that even when renin levels are low in the presence of triggers such as increased sodium concentration, aldosterone remains high, leading to hypertension and adverse cardiorenal outcomes.3,4
The cause of this feedback loop breakdown is unknown. However, risk factors may include excessive salt consumption, diabetes, sleep apnoea, adrenal adenomas, the presence of aldosterone-producing micronodules, and obesity—all conditions in which blood pressure regulation is disrupted.3,15,19,20 For example, adipose tissues release leptin, which bypasses the RAAS pathway to stimulate aldosterone secretion.19
The diverse roles of aldosterone in disease pathophysiology
Beyond fluid and pH regulation, aldosterone also promotes fibrosis by stimulating collagen production, causing scar tissue formation in the heart and blood vessels, and impairing function.4,21 Moreover, aldosterone can induce inflammation and oxidative stress, further contributing to damage in cardiovascular tissues.4,22,23 This indicates that beyond maintaining blood pH and electrolyte levels, aldosterone may also play a role in cardiovascular remodelling and renal function.21
There is also a newly discovered membrane receptor, the G protein–coupled oestrogen receptor (GPER), that binds to aldosterone and can mediate vasoconstriction, further sodium and water retention, and other risk factors for adverse health, such as cardiovascular endothelial dysfunction, apoptosis, and inflammation.24

An increasing body of evidence links aldosterone dysregulation and mineralocorticoid receptor hyperactivation to cardiovascular disorders like hypertension, metabolic syndrome, coronary artery disease, chronic kidney disease, and congestive heart failure.6
Increased aldosterone levels can also lead to off-target effects. In the endothelium for example, elevated aldosterone levels are correlated with increased inflammatory markers, stimulating fibrosis in the kidney, heart, and other vessels.21,23 Aldosterone can also make vessels less reactive to nitric oxide, which can lead to vascular dysfunction.3,4,25
Altogether, this inflammatory ecosystem further drives organ damage beyond hypertension alone, with the aldosterone-induced increased blood pressure leading to increased cardiorenal risk and the subsequent cardiorenal dysfunction resulting in end-organ damage independent of hypertension.3,4,25
Looking to the RAAS pathway for future therapeutic targets
The classical view of the RAAS pathway and aldosterone production is that of a hormonal feedback loop responsible primarily for sodium and water homeostasis.26 Our understanding of this loop has, however, greatly expanded, demonstrating that the roles of renin, aldosterone, and their associated substrates/ligands in human physiology may be more complex and far-reaching than originally thought. Current therapeutic options for treating hypertension consist mostly of angiotensin-converting enzymes (ACEs), angiotensin receptor blockers (ARBs), and mineralocorticoid receptor antagonists (MRAs).4 ACEs and ARBs cannot inhibit the hypersecretion of aldosterone, and their chronic use can result in the failure of aldosterone suppression, also known as aldosterone escape.4
Results from the PATHWAY-2 trial demonstrated that patients with aldosterone dysregulation see less of an effect receiving certain ARBs when compared to an MRA.27 These results suggest that a significant proportion (25%) of patients with hypertension would benefit from earlier treatment with a therapy that directly targets aldosterone.27 Though MRAs are effective in blocking aldosterone action, they are nonselective in nature and can lead to undesirable off-target anti-androgenic effects.28
Aldosterone synthase inhibition has been hypothesised as an alternative therapeutic option that is selective enough to prevent the off-target effects seen with MRAs.4 Suppressing aldosterone hypersecretion does not only play a role in preventing hypertension but also could prevent and reduce cardiorenal organ damage.3,4,25 Appreciating and further investigating the complex role of the RAAS pathway in the body is vital for both basic scientific research and the development of therapeutic interventions for a spectrum of cardiorenal diseases.


