Metabolism news and stories
Transforming clinical development in NASH
Clinical innovation
Home / Our therapy areas / Cardiovascular, Renal and Metabolism (CVRM) / Metabolism
When we eat, our body converts proteins, fats, and carbohydrates into energy, which can be used immediately or stored in fat, muscle or the liver.1 Metabolic disorders, often due to hormonal imbalances or genetic abnormalities, can disrupt the metabolism process, potentially leading to disease.1
Cardiometabolic diseases are a subset of metabolic diseases that specifically affect the cardiovascular system. Overweight/obesity and cardiometabolic diseases are deeply linked, with harmful fat accumulation significantly contributing to conditions like type 2 diabetes, hypertension, metabolic dysfunction-associated steatohepatitis (MASH), chronic kidney disease (CKD), heart failure and atherosclerotic cardiovascular disease (ASCVD).2-5 Understanding the interplay between risk factors and disease drivers is critical to improve outcomes for the hundreds of millions of people worldwide affected by these chronic diseases.6
Transforming clinical development in NASH
Clinical innovationOverweight/obesity and associated metabolic diseases, including type 2 diabetes and MASH, result in dysregulation across multiple organs and increase the risk of other related comorbidities.7 Through our research, which leverages our deep understanding of the interconnectedness of these chronic conditions, we have a unique opportunity to change the trajectory of rising trends in cardiometabolic diseases and improve quality of life.
Our research is focused on addressing the underlying mechanisms that link these complex conditions and contribute to increased morbidity and mortality. Clinical development of new solutions is accelerating to match the urgency of the large and growing unmet medical needs of patients with metabolic diseases. We aim to improve access globally to novel treatments for a broad population, including people living with overweight/obesity, type 2 diabetes, or serious liver conditions such as MASH.
Overweight/obesity is a complex, chronic, relapsing disease that affects 1 billion people globally and is projected to rise to 1.5 billion by 2035.8 Furthermore, overweight/obesity-related costs worldwide are estimated to surpass $4 trillion per year by 2035 if prevention and treatment measures do not improve.8 Overweight/obesity pathophysiology are intimately coupled with genetic, environmental, socioeconomic and behavioural factors and this is contributing to the growing epidemic of non-communicable diseases.2 This increasing burden requires urgent solutions.
Obesity is one of the top five risk factors for premature death and a driver of more than 200 comorbidities.9 More than 60% of people in the United States who are diagnosed with overweight/obesity have at least one of the following comorbidities:

To address the rising burden of these chronic conditions, a comprehensive approach must include the integration of overweight/obesity treatment as a central component of care. By targeting root causes and interconnected pathways, new therapies hold the potential to substantially lessen the collective burden on individuals, health systems and society.
As complex, chronic and heterogenous as these diseases are, new treatments alone will not solve the overweight/obesity crisis. Comprehensive and integrated care models that consider individual needs, preferences and underlying risk factors are essential for optimising health outcomes.
Our mission is to improve global access to cardiometabolic care options, by developing treatments for overweight/obesity that go beyond short-term weight loss, focusing on healthy weight management with better tolerability, organ protection and reduced cardiometabolic risk.

Overweight/obesity and insulin resistance are key drivers of type 2 diabetes and are also connected with the development of diseases of the heart and circulation, liver and kidneys.10 The global number of people living with diabetes is expected to rise to 783 million by 2045.11 People living with type 2 diabetes have an increased risk of developing several serious life-threatening health problems, resulting in lower quality of life and often facing high medical costs.12,13
We are committed to developing innovative solutions to ongoing treatment challenges, including oral options as an alternative to injectables, as well as combination therapies to potentially improve adherence and reduce pill burden. Additionally, we are engaging in research collaborations to develop cutting-edge treatments for type 1 diabetes, aiming to provide a growing patient population with innovative options to slow disease progression in a lifelong chronic condition on top of the current standard of care.

We are dedicated to addressing therapeutic gaps and improving health outcomes in cardiometabolic and liver diseases, which are also closely linked. In particular, liver cirrhosis is a chronic and progressive condition for which there is currently no cure.14 The limited treatments available are focused on reducing portal pressure, often a complication of liver cirrhosis, and alleviating symptoms.14
Emerging science suggests significant 'crosstalk' between the liver and other organs, reinforcing the need for a comprehensive approach to liver and cardiometabolic diseases that focuses on addressing root cause of disease and at all stages of disease progression.15
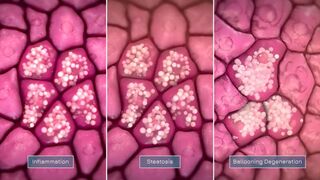
Metabolic dysfunction-associated steatohepatitis or MASH, is a liver disease in which a build-up of fat in the liver is followed by inflammation and cell damage.16 It is rapidly becoming a leading cause of chronic liver disease, with an estimated 350 million patients to be affected with fatty liver disease by 2030.17,18 People living with MASH are also at greater risk of requiring liver transplantation, hepatocellular carcinoma (HCC), type 2 diabetes and cardiovascular disease.19
While there are no direct markers of MASH, the primary disease drivers mirror those of overweight/obesity and type 2 diabetes, including lifestyle choices and dietary habits.20 Similarly, recent scientific discoveries have revealed strong genetic components predisposing individuals and certain populations to MASH, adding a new dimension to our understanding of this complex condition.21-24
Coupled with investments in cutting-edge technologies, we are researching treatments that address the metabolic, inflammatory, fibrotic and genetic drivers of MASH. We are using innovative approaches like precision medicine to develop targeted therapies that could offer more effective and personalised treatment options and prevent disease progression to cirrhosis or cancer. In an area of high unmet need with very limited treatment options, our aim is to identify the next wave of therapeutics that might offer unique benefits for these patients.
Across metabolism, our ambition is to reduce and reverse overweight/obesity and chronic cardiometabolic diseases, bringing together our heritage in understanding cardiovascular, renal and metabolic diseases with deep scientific capabilities. To do so, we are developing a portfolio of next-generation therapeutics – novel small molecules, drug combinations, cell and gene therapy, and advanced biologics such as dual-and-triple target peptides – which address multiple risk factors and tackle the underlying drivers of disease across cardiometabolic diseases.
As part of our long-term commitment to advancing innovative medicines for cardiometabolic diseases and overweight/obesity, we are engaging with partners who share in our commitment to pioneering science and can help bring these medicines to patients that need them.
Quell: Cell therapy for type 1 diabetes
Ionis: Precision medicine for MASH
SixPeaks: Novel targets for improved lean mass protection
1. Metabolic disorders. MedlinePlus. https://medlineplus.gov/metabolicdisorders.html. Updated August 23, 2016. Accessed 2024, August 19.
2. Lazarus E, Ortiz-Pujols S. Increasing clinical awareness of obesity as a serious, chronic, relapsing, and treatable disease. Am J Manag Care. 2022;28(15 Suppl):S271-S8.
3. Hsuan CF, et al. The waist-to-body mass index ratio as an anthropometric predictor for cardiovascular outcome in subjects with established atherosclerotic cardiovascular disease. Sci Rep. 2022;12(1):804.
4. Prasad R, et al. Chronic Kidney Disease: Its Relationship With Obesity. Cureus. 2022;14(10):e30535.
5. Volpe M, Gallo G. Obesity and cardiovascular disease: An executive document on pathophysiological and clinical links promoted by the Italian Society of Cardiovascular Prevention (SIPREC). Front Cardiovasc Med. 2023;10:1136340.
6. Disease GBD, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-59.
7. Ruze R, et al. Obesity and typer 2 diabetes mellitus: connections in epidemiology, pathogenesis, and treatments. Front End. 2023.
8. Federation WO. World Obesity Atlas 2024. https://data.worldobesity.org/publications/WOF-Obesity-Atlas-v7.pdf. Accessed: 2024, August 7.
9. Horn DB, et al. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359-75.
10. Rhodes Cea. Diabetes: Following the science in the search for a cure. https://www.nature.com/articles/d42473-021-00264-7. Accessed: 2024, August 7.
11. IDF. IDF Diabetes Atlas 2021. https://diabetesatlas.org/atlas/tenth-edition/ Accessed: 2024, August 7.
12. Staff MC. Type 2 Diabetes. https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/symptoms-causes/syc-20351193. Accessed:
13. Trikkalinou A, et al. Type 2 diabetes and quality of life. World J Diabetes. 2017;8(4):120-9.
14. NIH. Treatment for Cirrhosis. https://www.niddk.nih.gov/health-information/liver-disease/cirrhosis/treatment Accessed: 2024, August 7.
15. Ye DW, et al. Liver-adipose tissue crosstalk: A key player in the pathogenesis of glucolipid metabolic disease. Chin J Integr Med. 2017;23(6):410-4.
16. NIH. Definition & Facts of NAFLD & NASH. https://www.niddk.nih.gov/health-information/liver-disease/nafld-nash/definition-facts. Accessed: 2024, August 7.
17. Nature.com. Advances in MALSD/NAFLD. https://www.nature.com/collections/ggfhiijjac. Accessed: 2024, August 7.
18. Institute GL. What is Fatty Liver Day? https://www.international-nash-day.com/ Accessed: 2024, August 7.
19. European Association for the Study of the L, et al. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388-402.
20. Cheemerla S, Balakrishnan M. Global Epidemiology of Chronic Liver Disease. Clin Liver Dis (Hoboken). 2021;17(5):365-70.
21. He S, et al. A sequence variation (I148M) in PNPLA3 associated with nonalcoholic fatty liver disease disrupts triglyceride hydrolysis. J Biol Chem. 2010;285(9):6706-15.
22. Witzel HR, et al. PNPLA3(I148M) Inhibits Lipolysis by Perilipin-5-Dependent Competition with ATGL. Cells. 2022;12(1).
23. Romeo S, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet. 2008;40(12):1461-5.
24. Liu YL, et al. Carriage of the PNPLA3 rs738409 C >G polymorphism confers an increased risk of non-alcoholic fatty liver disease associated hepatocellular carcinoma. J Hepatol. 2014;61(1):75-81.
Veeva ID: Z4-68226
Date of preparation: September 2024